
Four Companies Wearing One Logo: The Architecture of Disconnection
$17 billion in restructuring. Same goals every cycle: simplify, delayer, speed up decisions. Why doesn't it stick? The problem isn't people. It's architecture.


Novo Nordisk: $1.25 billion in targeted savings. Pfizer: $7.7 billion. Bayer: €2 billion. Bristol Myers Squibb: $3.5 billion. Merck: $3 billion.
Over the past eighteen months, the industry's largest companies have announced savings targets totaling more than $17 billion and affecting tens of thousands of roles.
The stated goals are identical across every announcement: simplify the organization, improve decision-making speed, reduce layers.
I've heard this language before. Multiple times. At multiple companies. Because this isn't new.
The industry has cycled through this at least four times in fifteen years: 2010-2012, 2015-2018, 2020-2022, and now 2024-2025. Each wave sweeps through the major players—Roche, AstraZeneca, Novartis, Pfizer, Sanofi, AbbVie, Merck, and others—with tens of thousands of positions affected industry-wide. The press releases change dates. The language doesn't.
These savings targets exist for a reason beyond cost discipline. They're supposed to flow through to operating margins, the metric that analysts watch, that boards scrutinize, that ultimately determines whether efficiency rhetoric becomes financial reality.
And here's where it gets interesting.
Gross margins across big pharma remain healthy: 70 to 80 percent for most major players. That's pricing power. That's the product portfolio doing its job.
But by the time you account for R&D (20 to 25 percent of revenue) and SG&A (another 25 to 30 percent), operating margins land at 15 to 25 percent. Lower for some. The gap between what the products earn and what the organization keeps is staggering.
Billions in announced savings. Year after year. Cycle after cycle. And yet, operating margins remain compressed. Pfizer's stated goal for its $7.7 billion cost program? "Return to pre-pandemic operating margins." Return to. Not exceed. Not transform. Return to where they were.
McKinsey's analysis of 100+ industry announcements shows over $7 billion in cost savings targets across the sector. The money is real. The question is whether it translates to sustained operational improvement or simply resets the baseline for the next cycle.
If short-term savings drove sustained operational efficiency, we'd see it in the numbers by now. We don't.
Why not?
Operating margin compression has multiple causes. R&D cost inflation. Pricing pressure from the IRA. Patent cliffs. Portfolio mix. These are real forces, and restructuring alone won't neutralize them.
But here's what restructuring claims to address: organizational complexity. Decision-making speed. Functional alignment. And on these fronts, the cycle keeps repeating.
Restructuring tends to focus on headcount and org chart. Not on the operating model itself. Not on how work flows across functions. Not on the architecture that fragments what should be integrated.
Savings happen. But the underlying structure, the one that creates friction, duplication, and delay, often remains untouched.
That structure is what we're examining today.
Where the Seams Show
Here's what restructuring typically doesn't touch: the fundamental way pharmaceutical companies are organized.
Most pharma companies are structured around functions. Clinical Development. Regulatory Affairs. CMC (Chemistry, Manufacturing, and Controls). Commercial. Each with its own leadership, its own budget, its own objectives, its own definition of success.
On paper, all functions serve the same goal: getting medicines to patients. In practice, they operate as separate companies that happen to share a logo.
Clinical optimizes for trial speed and data quality. Regulatory optimizes for submission readiness and agency relationships. CMC optimizes for process robustness and manufacturing reliability. Commercial optimizes for launch timing and market access.
Each function executes well within its domain. The problem emerges at the boundaries.
When a clinical timeline shifts, what happens to the CMC scale-up plan? When a regulatory strategy changes, who adjusts the commercial launch sequence? When manufacturing encounters a constraint, how quickly does clinical learn that their supply assumptions no longer hold?
The answer, more often than not: slowly. Painfully. After the fact.
Work queues at every handoff. Information degrades as it crosses functional lines. Assumptions made in one function go unvalidated by another until it's too late to adjust without cost and delay.
This isn't a coordination failure in the sense of people not trying. It's an architectural reality. The organization is designed for functional excellence. Cross-functional integration is an afterthought, bolted on through committees, matrix reporting lines, and coordination overhead.
A McKinsey 2024 survey of 50 global life sciences leaders found that only one in five believe their current operating model enables timely decision-making at the appropriate organizational levels. Four in five do not.
That's not a people problem. That's a structure problem.
Archaeological Sites
This structure didn't emerge by accident. It evolved.
Most large pharmaceutical companies are archaeological sites. Layer upon layer of organizational decisions, accumulated over decades.
Merck today isn't one company. It's the legacy of Merck, Schering-Plough, Organon, and dozens of smaller acquisitions, each with their own systems, cultures, and ways of working. Pfizer carries the organizational DNA of Warner-Lambert, Pharmacia, Wyeth, and more recently, Seagen. Bristol Myers Squibb absorbed Celgene. AbbVie split from Abbott and acquired Allergan.
Different IT systems. Different planning processes. Different definitions of what "stage gate" means. Different expectations for how functions interact.
Integration efforts focus on the obvious: consolidating facilities, eliminating redundant roles, harmonizing compensation structures. The savings announcements we see today are often the tail end of this work.
But integration rarely reaches the operating model itself. How work actually flows from discovery through development through manufacturing through launch. That architecture tends to survive intact, with each legacy organization's functional boundaries preserved beneath a unified org chart.
So the pattern repeats. Each iteration treats symptoms—too many people, too many layers, too much cost—without addressing the underlying architecture that generates those symptoms.
You can redesign the org chart without redesigning how work flows. Most companies do exactly that.
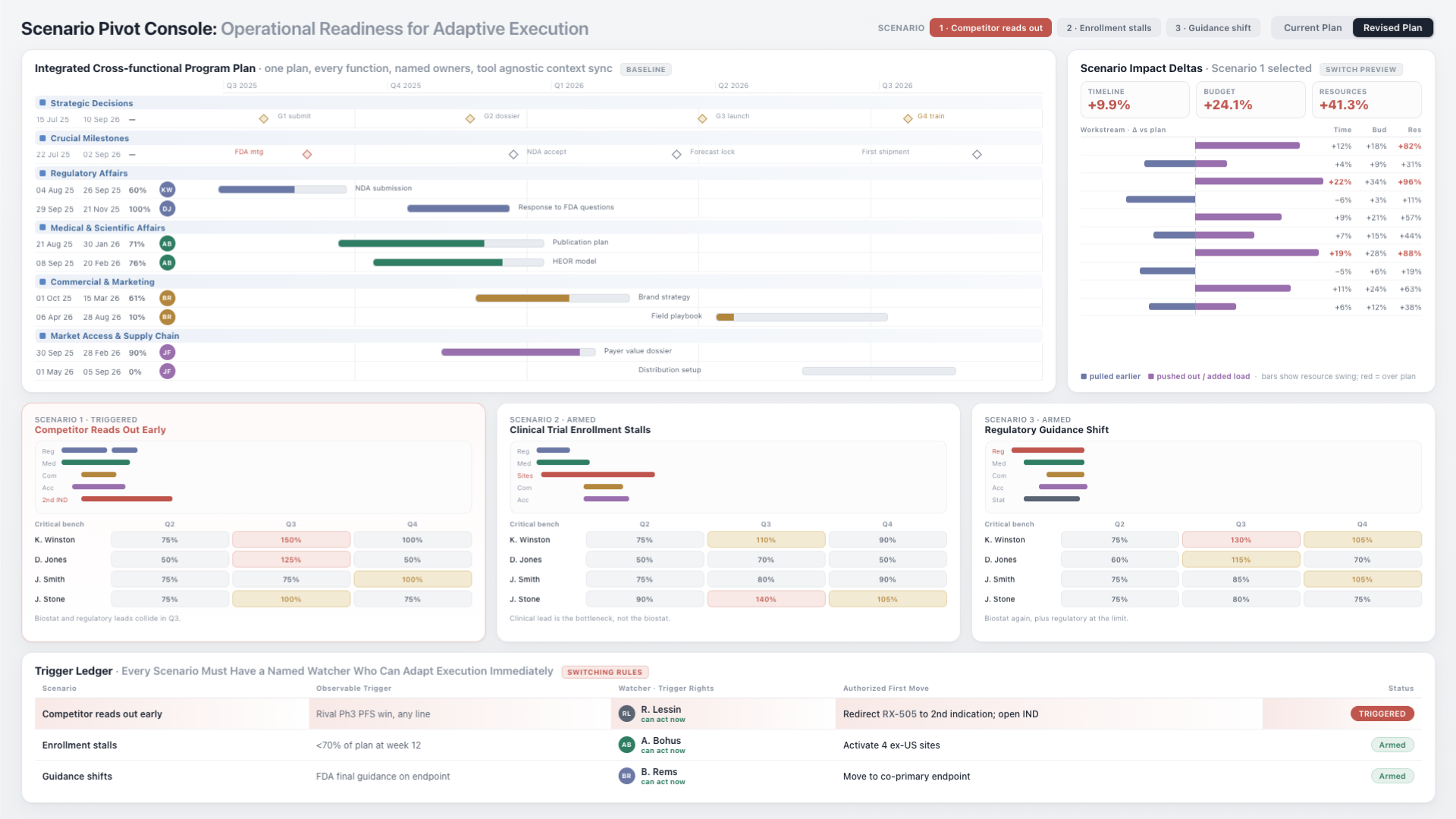
Four Clocks, No Timekeeper
The architecture problem runs deeper than org charts and reporting lines.
Each function in a pharmaceutical company operates on a different clock, with a different definition of success, and a different relationship with risk.
Clinical Development thinks in trial phases. Eighteen months to first patient in. Thirty-six months to database lock. Their clock is driven by enrollment curves and data maturation.
Regulatory Affairs thinks in submission windows and agency cycles. Their clock is driven by guidance documents, review timelines, and the rhythm of FDA and EMA interactions.
CMC thinks in process development milestones, technology transfers, and validation campaigns. Their clock is driven by manufacturing scale-up and the physics of producing drug product at quality.
Commercial thinks in launch windows, payer negotiations, and competitive dynamics. Their clock is driven by market access timelines and the revenue implications of every month of delay.
Four functions. Four clocks. Four definitions of what "on time" means.
Four clocks. No timekeeper. And everyone is surprised when the trains run late.
Now here's the root cause: there is no structural owner of the white space between these functions.
Each function owns its deliverables. No one owns the integration. No one owns the handoffs. No one owns the dependencies that connect a CMC timeline to a regulatory submission to a commercial launch.
That white space, where information should flow, where assumptions should be validated, where schedule risks should surface, is architecturally homeless. It gets managed through meetings, through project management overlays, through sheer force of will by program leaders who have responsibility but often lack authority.
The organization is designed for functional depth. The gaps between functions are left to ad hoc effort. And ad hoc effort doesn't scale.
The Coordination Tax
This architectural fragmentation has costs. Real ones. Measured in time, money, and outcomes that matter.
When functions operate on different clocks without structural integration, schedules slip. Not dramatically, not in ways that make headlines, but persistently. A few weeks here. A month there. Delays that compound across handoffs until the gap between "when we could have filed" and "when we actually filed" stretches to quarters, sometimes years.
Tufts Center for the Study of Drug Development estimates that a single day of delay costs $500,000 to $800,000 in unrealized revenue for a typical pharmaceutical product. That's not a rounding error. That's a math problem that accumulates silently while functions wait for alignment that the architecture doesn't provide.
But the financial cost isn't the real cost.
The real cost is measured in patients.
Research has shown that a treatment delay as short as four weeks can measurably increase mortality in oncology. Patients with life-threatening conditions are optimizing for survival while organizations are navigating internal handoffs.
Consider what happens after FDA approval. The regulatory milestone is met. The organization celebrates. But the patient can't access the medicine yet.
Release testing. Quality disposition. Labeling and packaging. Distribution qualification. Payer negotiations. Formulary placement. Each step owned by a different function, each with its own timeline, each waiting for inputs from another.
The result: an average gap of 63 or more days between FDA approval and the first prescription reaching a patient in the United States.
Not all of that gap is waste. Release testing takes time. Quality disposition is real work. Distribution qualification serves patients.
But when Gilead launched Livdelzi within hours of approval, they proved that most of that gap isn't the work itself. It's the waiting. Waiting for handoffs. Waiting for alignment. Waiting for work that could have been done in parallel but wasn't.
Two months of patients waiting for a medicine that already exists, already works, already has regulatory blessing. That's not a scientific limit. That's a coordination tax.
Designing for Flow
The implication is clear: restructuring headcount without restructuring the operating model is treating symptoms while the underlying condition persists.
What would a different approach look like?
It would start by recognizing that functional excellence and enterprise integration are not the same thing. You can have world-class clinical operations, world-class regulatory affairs, world-class manufacturing, and world-class commercial execution, and still have a fragmented organization if those functions aren't architecturally connected.
The shift required is from designing for functional depth to designing for cross-functional flow.
This doesn't mean abandoning functional expertise. Clinical scientists should still own clinical science. Regulatory strategists should still own regulatory strategy. Manufacturing engineers should still own manufacturing.
But the architecture needs to change. The white space between functions, where handoffs happen, where dependencies live, where schedule risk accumulates, needs to become a first-class design consideration. Not an afterthought. Not a layer of meetings and status updates. A structural element of how the organization operates.
Some companies have experimented with this. Eli Lilly's CHORUS model, originally designed for early clinical development, demonstrated what becomes possible when small, cross-functional teams operate with end-to-end ownership of an asset. The results were striking: 3x faster timelines, development costs at one-sixth the traditional level, Phase II success rate of 54% compared to 29% for traditional development.
But CHORUS remained confined to early development. It didn't scale to late-stage trials. It didn't transform Lilly's entire operating model. Successful molecules graduated back into the traditional functional structure for Phase III and beyond.
The model proved the concept works for a specific, bounded scope. The question is whether the principles can be adapted across the full lifecycle, or whether the barriers that prevented CHORUS from scaling reveal something fundamental about the difficulty of this transformation.
Architecture, Not Org Charts
If the solution were easy, it would already be widespread. It isn't. There are real barriers.
Functional organizations persist because they work, up to a point. They create clear accountability. They develop deep expertise. They simplify management. A clinical leader knows exactly what they own. A regulatory leader knows exactly what they own. That clarity has value.
Cross-functional integration creates ambiguity. Who owns the dependency between CMC and regulatory? Who owns the gap between clinical data lock and commercial launch readiness? When something falls between functions, who is accountable?
Most organizations answer this question with matrix structures. Dual reporting lines. Employees reporting to both functional and project managers. The intent is integration. The reality is often confusion over roles, power struggles between managers, communication breakdowns despite increased meetings, and employee burnout from competing demands.
McKinsey's survey found that 50% of pharma companies haven't started implementing agile cross-functional initiatives or are only in early stages. Those that have tried face predictable challenges: departmental silos persist beneath the matrix overlay, functional managers protect their resources, project managers lack authority to make decisions stick, and the added coordination overhead can slow things down rather than speed them up.
The standard organizational responses, more meetings, more alignment sessions, more coordination layers, often add bureaucracy without clarity. Integration becomes overhead rather than architecture.
The path forward requires something different: architecture that makes cross-functional flow visible without adding burden.
Some organizations have demonstrated this is possible. Johnson & Johnson's supply chain transformation offers one model: end-to-end visibility across pharmaceutical, medical device, and consumer divisions, with real-time tracking from supplier to customer. The World Economic Forum has recognized seven J&J manufacturing sites as "Lighthouses"—more than any other company—for their integration of cross-functional data flows. The principle that emerged: when information flows easily across boundaries, operators and managers can focus on making products rather than chasing status.
The technology to enable this kind of visibility now exists. The question is whether organizations will use it to redesign the architecture, or simply add another layer on top of the old one.
The Question
The restructuring announcements will continue. The savings targets will be met. The headcount will adjust. The org charts will be redrawn.
And in two to three years, we'll likely be here again.
Unless something different happens.
The pharmaceutical industry has mastered functional excellence. The science has never been better. The regulatory pathways have never been clearer. The commercial capabilities have never been more sophisticated.
What remains unmastered is the integration. The white space. The architecture that connects four companies into one.
The models exist. CHORUS proved that cross-functional teams with end-to-end ownership can move three times faster at one-sixth the cost. J&J demonstrated that enterprise-wide operational visibility is achievable at scale. The technology exists. The evidence exists.
And yet.
Four decades of restructuring. Four cycles in fifteen years. Billions in announced savings. The same stated goals appearing in press release after press release: simplify the organization, improve decision-making speed, reduce layers.
Why doesn't it stick?
That's the question this industry keeps avoiding. Not how to restructure—we know how to restructure. But why, when everyone sees the problem, does no one solve it?
We know how to restructure. What we don't know is how to stop needing to.
The answer, I suspect, has less to do with operating models and more to do with what happens to the people who try to change them. The architecture problem is real. But beneath it lies something about accountability and exposure that we'll need to examine more closely.
Patients are waiting. The science is ready. The architecture could catch up.
The question is whether we're willing to talk about what's actually in the way.
References
- McKinsey & Company. "Simplification for success: Rewiring the biopharma operating model." McKinsey Life Sciences Practice, March 2025. mckinsey.com
- Tufts Center for the Study of Drug Development. "Cost of Developing a New Drug." CSDD Impact Reports, 2024. csdd.tufts.edu
- Hanna TP, King WD, Thibodeau S, et al. "Mortality due to cancer treatment delay: systematic review and meta-analysis." BMJ, 2020. pubmed.ncbi.nlm.nih.gov/31566658
- Owens PK, Raddad E, Miller JW, et al. "A decade of innovation in pharmaceutical R&D: the Chorus model." Nature Reviews Drug Discovery, 2015. nature.com/articles/nrd4536
- Pfizer Inc. "Pfizer Reports Fourth-Quarter and Full-Year 2024 Results." Pfizer Investor Relations, January 2025.
- Novo Nordisk. "Capital Markets Day 2024: Strategic Update." Novo Nordisk Investor Relations, 2024.
- Merck & Co. "Merck Announces Global Workforce Restructuring." Merck Investor Relations, July 2025.
Further Reading
From Unipr Insights:
- Reflections on JPM 2025: The Era of Operational Excellence — Why operating margins have become the defining metric for pharmaceutical performance
- Why Connecting Data Isn't Enough: The Coordination Imperative — The difference between connected systems and coordinated operations
- Same Day Launch: Future Blockbusters Needn't Leave Money on the Table — What enables launches within hours of approval
- Global Launch Delays: Impact on Patients & Revenue — The human and financial cost of coordination gaps
- The $25B AI Paradox: Why Pharma is Missing Its Biggest Opportunity — The gap between discovery AI investment and operations AI neglect

Compliance
Unipr is built on trust, privacy, and enterprise-grade compliance. We never train our models on your data.




Start Building Today
Log in or create a free account to scope, build, map, compare, and enrich your projects with Planner.